
By Dayo Adesulu
In Nigeria, access to healthcare is not merely a policy challenge—it is a matter of life and death. Across both urban centers and rural communities, millions of citizens face an agonizing reality: hospital shelves are often empty, genuine medications are scarce, and the cost of treatment is beyond the reach of the average Nigerian.
According to the National Bureau of Statistics (NBS), over 133 million Nigerians are classified as multidimensionally poor. This includes lack of access to healthcare, education, clean water, and adequate nutrition. Economic hardship directly correlates with poor health outcomes, with high maternal and child mortality rates and a resurgence of preventable diseases like malaria, tuberculosis, and typhoid fever.
A Two-Front Crisis: Poverty and Counterfeit Drugs
Take Ibrahim from Nasarawa, a subsistence farmer who earns less than ₦500 a day. When his daughter was diagnosed with malaria, the public hospital had no antimalarial medication. He was directed to a private chemist where he spent over ₦3,500—only to discover later that the drugs were fake.

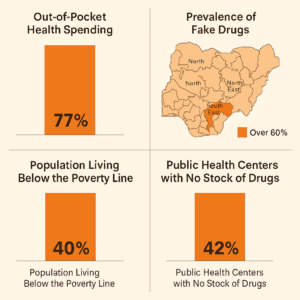
The World Health Organization (WHO) estimates that 42% of all fake medicines reported globally between 2013 and 2017 were found in Africa, with Nigeria being one of the most affected. According to the National Agency for Food and Drug Administration and Control (NAFDAC), over 17% of pharmaceutical products in circulation in Nigeria are substandard or falsified.
- WHO Launches Free Cancer Drug Initiative for Children in Low-Income Nations
- https://crediblenews.com.ng/quota-or-injustice-the-deepening-divide-in-n/
The implications are dire: fake drugs not only fail to treat illnesses but often exacerbate conditions, leading to long-term disability or death. In 2018 alone, the Federal Ministry of Health estimated that over 10,000 deaths in Nigeria were directly linked to counterfeit medications.
“The Cost of a Cough”
“My son started coughing at night, and by morning he couldn’t breathe properly,” said Amina Bello, a 34-year-old petty trader in Kano. “At the government hospital, the doctor wrote a prescription, but the pharmacist said they had run out. I went to a local chemist and bought what I could afford.”
Two days later, her four-year-old son, Yusuf, died of pneumonia—untreated because the syrup she bought was counterfeit.
Amina never got justice. “I still carry the bottle with me. It says ‘Made in India,’ but no NAFDAC number. I just want answers. I want people to know these fake drugs kill us slowly.”
Stories like Amina’s are far too common. In 2021 alone, Médecins Sans Frontières (MSF) reported a 30% increase in pneumonia-related child deaths in northern Nigeria, attributing many to delayed care and drug quality failures.
“The Cost of Survival in the City”
Chinedu Okonkwo, a 52-year-old schoolteacher in Lagos, was diagnosed with type 2 diabetes in 2022. At first, he followed all medical advice—regular clinic visits, insulin shots, and dietary changes. But within a year, the cost of his medication had nearly doubled.
“I used to spend ₦15,000 per month on drugs. Now it’s ₦32,000, and my salary hasn’t changed,” Chinedu said. “I had to stop going for tests. I even reduced my insulin dose to make it last longer.”
By mid-2024, he suffered a minor stroke and partial vision loss. Doctors said it was due to unmanaged sugar levels. When asked why he didn’t buy from a cheaper outlet, Chinedu replied, “You can’t tell which ones are fake. I don’t want to die from poison instead of the disease.”
His story mirrors that of many middle-income Nigerians who now face impossible trade-offs: food or medicine, rent or survival.

Rural Areas: The Forgotten Frontier
In rural communities across states like Zamfara, Ebonyi, and Benue, health centers are often the only option for miles. Yet these facilities routinely lack trained personnel, essential drugs, or basic equipment.
A 2022 assessment by the Nigerian Primary Health Care Development Agency (NPHCDA) revealed that over 70% of primary health care centers (PHCs) in rural Nigeria lacked electricity, clean water, or essential drugs.
“I had to walk 11 kilometers to reach the nearest clinic,” recounts Blessing, a pregnant woman from a village in Cross River. “When I arrived, they had no folic acid, no paracetamol, nothing. They told me to come back in a week.”
The United Nations Population Fund (UNFPA) reports that Nigeria accounts for nearly 20% of global maternal deaths, many of which occur in remote rural areas where access to emergency obstetric care is severely limited.
Dr. Hadiza Abubakar, a community nurse in rural Kaduna, shares the burden: “There are days I can only give advice, not medicine. How do you look a mother in the eyes and tell her to find money for drugs you know she can’t afford? It breaks us. We are trained to save lives, not watch them slip away.”
Urban Realities: Better Infrastructure, Same Injustice
Even in urban centers like Lagos, Abuja, and Port Harcourt—where hospitals are better equipped—the system is stretched thin. While consultation may be free or subsidized in government facilities, patients still pay out-of-pocket for lab tests, scans, and nearly all medications.
According to a 2024 survey by NOI Polls, 61% of urban residents had, at some point, opted for self-medication due to the unaffordability of hospital-prescribed drugs. Additionally, over 80% of Nigerians rely on out-of-pocket spending for healthcare, making Nigeria one of the countries with the highest healthcare out-of-pocket expenditures in Africa.
Lessons from Africa: What Nigeria Can Learn from Its Neighbors
While Nigeria remains Africa’s largest economy, it lags behind in delivering basic healthcare. In contrast, some smaller African countries have implemented reforms that Nigeria can learn from—and possibly surpass.
Ghana: National Health Insurance That Works
Ghana launched its National Health Insurance Scheme (NHIS) in 2003. Unlike Nigeria’s limited NHIS, Ghana’s version now covers over 55% of the population, including informal sector workers. The scheme is funded by a value-added tax (VAT) and managed through decentralized community-based structures.
Result: Infant mortality dropped by 30%, and immunization coverage rose to 90% between 2008 and 2019.
Rwanda: Turning Tragedy into Transformation
Following the 1994 genocide, Rwanda rebuilt its healthcare system from the ground up. Its Mutuelles de Santé—a community-based health insurance program—now covers over 90% of the population.
Key to its success:
- Strong central regulation
- Public-private partnerships
- Investment in health data systems and local pharmaceutical production
Result: Rwanda now has one of the lowest maternal mortality rates in Sub-Saharan Africa.
Dr. Chikwe Ihekweazu, former Director-General of the Nigeria Centre for Disease Control (NCDC), once noted:
“Our challenge is not knowledge or funding—it’s accountability.”
The Role of Government and Regulation
Despite repeated promises, government spending on health remains far below international benchmarks. In 2023, Nigeria allocated just 5.7% of its national budget to the health sector—well below the 15% commitment agreed upon in the 2001 Abuja Declaration.
The result? Weak enforcement of drug quality regulations, a porous border system, and a thriving black market for counterfeit drugs. The Pharmaceutical Society of Nigeria (PSN) reports that less than 30% of drugs consumed in the country are produced locally, leaving the rest to be imported, often with minimal oversight.
What Can Be Done?
- Subsidize Essential Medicines: Federal and state governments must increase funding to make essential drugs available at all public hospitals, especially at the PHC level.
- Strengthen NAFDAC: Equip the agency with advanced technology like drug authentication devices (TRUSCAN), expand mobile labs, and recruit more trained personnel.
- Enforce Price Regulation: Implement and enforce a national drug price control mechanism to prevent price gouging in pharmacies and hospitals.
- Revive Local Manufacturing: Provide tax incentives and funding to domestic pharmaceutical companies to produce high-quality, affordable medications.
- Public Education: Launch aggressive nationwide campaigns to educate citizens on the dangers of fake drugs and the importance of verifying medications.
Conclusion: The Price of Neglect
From Chinedu’s insulin cuts in Lagos to Blessing’s 11-kilometer walk in Cross River, the message is clear: Nigeria’s healthcare system is not broken—it is being abandoned. The sick are not only battling illness; they are fighting a system designed to fail them if they are poor, rural, or simply unlucky.
In a country that boasts one of Africa’s largest economies, it is an outrage that children die for lack of ₦500 cough syrup, that women give birth in candlelit clinics, and that honest nurses offer prayers instead of penicillin.
This is not just a health crisis—it is a moral one.
Call to Action: A Country Cannot Thrive While Its People Die
Nigeria must choose to care. Government officials must realize that health is the foundation of productivity, prosperity, and peace. We call on the Federal Ministry of Health, NAFDAC, and lawmakers at every level to:
- Fully fund and transparently implement the Basic Health Care Provision Fund.
- Hold counterfeit drug distributors criminally accountable—with no exceptions.
- Expand health insurance to include informal workers, market women, and farmers.
- Rebuild trust in hospitals by making essential drugs free, real, and available.
To do less is to sentence millions to slow, silent deaths.
Let this article be a record, a reckoning, and a rallying cry—because health is not a privilege. It is a human right.
#HealthcareInNigeria, #AccessToMedicine, #PovertyAndHealth, #FakeDrugsKill, #ReformHealthcareNow,